Physical Examination for
Shoulder
Anthony Luke MD, MPH
Examination
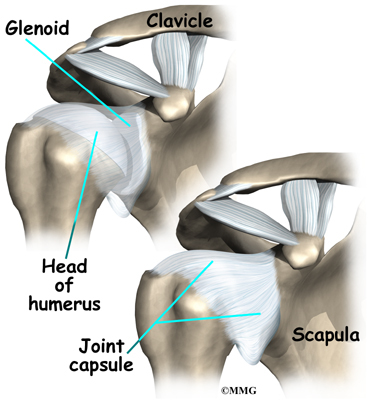
The glenohumeral joint is the most mobile
joint in the body, but the large multi-directional range of motion is a
trade-off for joint stability. The lack of stability makes the shoulder more
susceptible to a large spectrum of injuries, especially with overhead activities
involved in sports such as baseball, volleyball, swimming and weight lifting.
The shoulder girdle is important because is serves as the connecting joint
between the arm and the axial skeleton. It serves as the base of support for
movements occurring at the elbow, wrist and hand.
During an examination, taking a thorough
history is as important as the physical exam itself. The clinician should
inquire about the patient’s hand dominance, as well as their occupation and
recreational activities. It is also important to establish their chief
complaint, which may include pain, instability, weakness, or loss of range of
motion. Complaints of numbness and tingling may be associated with
neurovascular disorders, and stiffness may suggest adhesive capsulitis and/or arthritis.
Furthermore, any crepitus may indicate bursa, osteoarthritis or rotator cuff
pathology. It is also important to have patients try and establish an
approximate timeline for when the injury occurred and what event or mechanism,
if any, lead to the injury or onset of symptoms. For patients who report a
dislocation, it should be asked what position the arm was in at the time of the
dislocation, and what the frequency of dislocations or subluxations were.
Finally it is important to establish what type of activities of daily living
the patient can and cannot perform. Such activities include simple everyday
tasks like getting dressed, lifting an object overhead, sleeping on the
shoulder, brushing your teeth, combing your hair, putting on shoes, and carrying
or lifting objects like groceries.
Paplation
There are several important bony and soft
tissue structures that need to be palpated during the shoulder physical exam.
Bony structures should include: the sternoclavicular joint, the clavicle, the
acromioclaviular joint, the coracoid process, the borders of the scapula, and
the greater and lesser tuberosities of the humerus. Soft tissue landmarks
should include: the subacromial bursae, the supraclavicular fossa, the long
head of the biceps tendon, the trapezius, and other associated muscles and
tendons.
Range
of Motion
Active range of motion performed by the
patient is typically assessed first, and can be affected by both pain and motor
function. The patient can be either seated or standing during the assessment,
and movements to be tested should include forward flexion, extension,
internal/external rotation, and abduction/adduction.
Active
Range of Motion: Forward Flexion and External Rotation
Active
Range of Motion: Internal Rotation
Passive range of motion is performed by the clinician with the patient seated or supine in the same planes previously stated. This is used to isolate motion for an accurate evaluation of soft tissue.
Passive range of motion is performed by the clinician with the patient seated or supine in the same planes previously stated. This is used to isolate motion for an accurate evaluation of soft tissue.
Passive
Range of Motion: Horizontal Adduction
Normal motion for forward flexion is considered
to be 0° to 170-180°, while normal extension is said to be 60°. For internal
and external rotation, the arm should be abducted to 90° for an accurate
measurement. Normal internal rotation is said to be 90°, while normal external
rotation is around 60-70°. It is important to keep in mind that these values
can vary greatly with patients who are overhead athletes, such as baseball or
softball players. For adduction, the assessment is normally limited due to the
trunk, but typically 30° is considered normal. Abduction motion can range from
0° to 180°
An example of limited passive range of motion
can be seen in cases of frozen shoulder.
Frozen
Shoulder: External Rotation
To improve range of motion, special exercises
such as Codman’s Pendulum can be performed to help relax the muscles around the
shoulder, reduce pain, and increase motion.
Codman’s
Pendulum
Have the patient standing in a relaxed
position, and tell them to swing their weak arm in a circular motion while
keeping their shoulder nice and relaxed. Be sure they swing their arm in both
the clockwise and counterclockwise directions.
Rotator
Cuff Strength Testing:
Empty
Can Test
Description: The empty can test is used to evaluate
the strength and integrity of the supraspinatus muscle and tendon.
Maneuver: Have the patient stand with their
shoulder abducted to 90° and horizontally adducted forward 30° with the thumbs
pointing down towards the floor, as if they are pouring out a can. Ask the
patient to maintain this position. Proceed to apply downward resistance to the
patient’s forearm. A variation of this test can be done at 30° abduction
instead of 90°, where the supraspinatus should function in relative isolation.
Positive
findings: Decreased strength
or pain on resisted testing.
External
Rotation
Description: The external rotation test examines the
strength of the infraspinatus and teres minor.
Maneuver: With the patient’s arms at their side,
externally rotated 45° and elbow flexed to 90°, the examiner applies an
internal rotation moment to assess the strength of the external rotators.
Positive
Findings: Decreased strength
or pain on resisted testing. Significant weakness of the infraspinatus may be
indicative of suprascapular nerve palsy, where the infraspinatus become
denervated. This can be due to trauma, ganglion cyst or illness.
Subscapularis
Lift-Off Test
Description: The lift off test evaluates the muscular
strength of the subscapularis.
Maneuver: With the patient seated or standing,
have them internally rotate their arm behind their back. Then ask the patient
to lift the back of their hand off their lower back. If they are unable to
complete this task, apply resistance to the palm to assess the strength of the
subscapularis.
Positive
findings: Inability to lift
the dorsum of hand off the back.
Impingement/Rotator
Cuff Special Tests:
Neer’s
Impingement
Description: The Neer impingement test assesses the
presence of impingement of the rotator cuff, primarily the supraspinatus, as it
passes under the subacromial arch during forward flexion.
Maneuver: Stabilize the scapula with one hand
while applying passive forced flexion of the arm.
Positive
findings: Pain in the
anterior shoulder or reproduction of the patient’s symptoms.
Hawkin’s
Kennedy Impingement Test
Description: The Hawkin’s test is used to evaluate
impingement of rotator cuff and subacromial bursa.
Maneuver: The patient is seated or standing and
with their arm forward flexed to 90°and their elbow bent to 90°. Stabilize the
top of he shoulder while internally rotating the arm at the forearm.
Tip: Stand at the side of the patient with
one hand on top of the shoulder and keep the patient from elevating the
shoulder. The other hand should be positioned close to the elbow with the thumb
down, making it more comfortable for the examiner to internally rotate the arm.
The test should not be done with the arm abducted.
Positive
Findings:Pain in the anterior
shoulder or reproduction of the patient?s symptoms with the test.
Instability
Special Tests:
Load
and Shift Test
Description: The Load and Shift test examines
integrity of shoulder stability in the anterior and posterior directions.
Maneuver: Have the patient seated or supine with
their arm relaxed and resting at their side. Grasp the head of the humerus with
thumb and fingers and apply an anterior and posterior glide from the resting
position.
Positive
Findings: Excessive gliding
of the humeral head is considered to be a positive test. The degree of
stability can be graded based on the following: Grade 0 is no gliding from the
center of the glenoid, Grade 1 equals translation to the glenoid rim, Grade 2
translation of the head over the glenoid rim but no locking, and Grade 3
results in the head of the humerus locking over the glenoid rim.
Apprehension
Relocation
Description: The apprehension test, described by Row
and Zarin, tests for anterior instability of the shoulder. The relocation test,
described by Jobe, is used in conjunction with the apprehension test to
distinguish between anterior instability and primary impingement of the
shoulder.
Maneuver: : To perform the apprehension test, have
the patient supine, with their arm abducted and elbow flexed to 90°. Gently
externally rotate the arm. Once the patient becomes apprehensive or complains
of pain, proceed with the relocation and surprise test by applying a posterior
force to the humeral head.
Positive
Findings: For the
apprehension test, the patient may complain of pain or be apprehensive that
their arm may dislocate as it is externally rotated. The relocation test is
positive if the symptoms of apprehension reduce, or if the clinician is able to
externally rotate the shoulder further without any increase in pain or
apprehension. If the symptoms persist following the posterior directed force,
the pain is associated with primary impingement and not anterior shoulder
instability.
Sulcus
Sign
Description: The sulcus sign tests for inferior
instability caused by laxity of the inferior glenohumeral ligament complex.
Maneuver: : Have the patient seated with their arm
resting at their side. Grasp the patient’s upper arm and apply a distal force
to it.
Positive
Findings: Increased inferior
movement of the humeral head or the visible development of a sulcus at the
glenohumeral joint are positive findings. A positive test can often suggest
that the patient has multidirectional instability, espeically if there are
other signs of join instability.
Labral
Special Tests:
O’Brien’s
Test
Description: This test examines the integrity of the
glenoid labrum and the acromioclavicular joint.
Maneuver: With the patient seated or standing,
instruct the patient to raise their arm into 90° of forward flexion with their
elbow extended, and then adduct their arm 10-15°. Have the patient internally
rotate their arm and point their thumb down to the ground. Apply a downward
force to the arm. Then instruct the patient to externally rotate their arm and
point their thumb towards the ceiling. Again, apply a downward force.
Alternate
View:
Positive
Findings: Positive findings
for labral pathology occur when the first test reproduces pain, while the
second test decreases or eliminates pain. The pain associated with labral tears
is described as being deep in the shoulder. Pain situated over the
acromioclavicular joint is associated with acromioclavicular joint pathology
such as osteoarthritis or a shoulder separation, rather than labral pathology.
Pain in the AC joint is usually equal with the palm down or the palm up.
.jpg)









.jpg)

